Tina and I slept solid last night. We needed the rest. Big day today.
We’re meeting the surgeon that will probably be taking care of our little girl. The only reason I say probably is because I had to leave the door open a bit just in case something isn’t right. I’m 95% sure this is our guy, but we still need to see him in person to be sure.
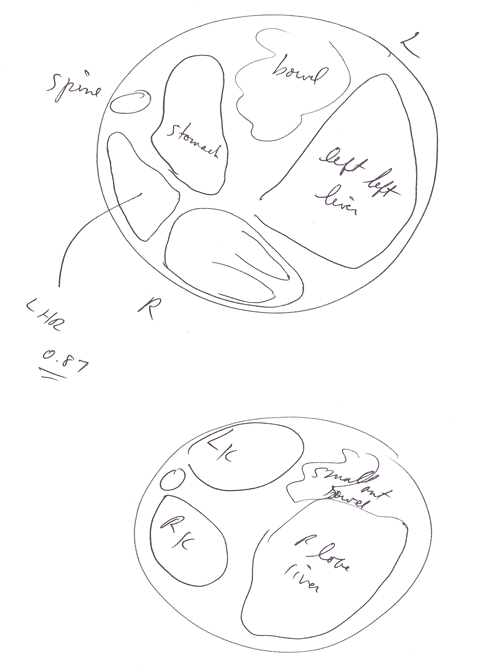 We drive over to the hospital to initially meet with the OBGYN that will be delivering our baby – Dr. Richards. Right from the beginning I felt good about this guy. He was very genuine in his words and had fantastic “bedside manner”. He performed an ultrasound on Tina as well, confirming a lot of what we already knew. He also gave us some more insight into the location of our baby’s organs. He drew us a simple diagram (see picture) that showed what was in the chest, and what remains in the belly. So far so good. No red flags with Dr. Richards. In fact, I’m feeling good that he’ll be the one delivering the baby.
We drive over to the hospital to initially meet with the OBGYN that will be delivering our baby – Dr. Richards. Right from the beginning I felt good about this guy. He was very genuine in his words and had fantastic “bedside manner”. He performed an ultrasound on Tina as well, confirming a lot of what we already knew. He also gave us some more insight into the location of our baby’s organs. He drew us a simple diagram (see picture) that showed what was in the chest, and what remains in the belly. So far so good. No red flags with Dr. Richards. In fact, I’m feeling good that he’ll be the one delivering the baby.
After meeting with him we call to confirm the meeting location with Dr. Kays. Tina and I take the shuttle over to another part of the hospital. Our meeting with Dr. Kays is scheduled for 1pm so we grab a quick bite to eat in the hospital. Fortunately we’re not just limited to the cafeteria due to the fact that there’s also a Wendy’s in the hospital as well. This is a good thing considering how much time we’ll be spending there.
We have trouble locating where to meet the Dr. so we call his assistant. She sends an intern down to direct us to a conference room where we’ll be meeting Dr. Kays. In the room there are a couple magazines on the table. One of them is from the University, highlighting the work of Dr. Kays. I leaf through the article and read this story of a couple that went through almost exactly what we’re going through.
They experienced the hopelessness of a local hospital and didn’t know where to turn. Their hope returned after meeting Dr. Kays. In everything I’ve read about Dr. Kays it seems one of the primary ingredients that he brings that most other Dr. / Hospitals don’t is genuine hope.
At about 1:45pm Dr. Kays comes through the door in the conference room. A little more grey than the picture in the article from 2002, but it’s the same guy nonetheless. We introduce ourselves and Dr. Kays begins to tell us everything we could want to know about our baby girl and her disorder.
He begins with details on the birth defect itself. What it is, and the complications surrounding it. How it occurs, which is still not totally known, and the different levels of severity. I’m incredibly focused on what he’s saying. I only wish I would have had a video camera to capture it all!
He then talks about specifics about our little girl and he lets us know that by the end of our meeting he’ll be able to give us a general idea of our baby’s chances. At least as best as a human can. He also indicates that he’ll be focusing on our baby’s brain as much as her lungs.
He asks for the drawing that Dr. Richards sketched out and for the ultrasound report. Dr. Richards had confirmed that we are looking at a .8 LHR (lung to head ratio), which is severe. This is something the other doctors were able to tell us as well, so this was no surprise. What was a surprise though was how he reacted to that news.
He began to explain that the LHR is just one component that measures the chances of surviving but there are so many other variables involved. This is what makes CDH so challenging because the smallest tweak of a respirator, the timing of giving the proper drugs, knowing if and when to use ECMO, all play into our baby getting better.
Most doctors will treat the baby’s condition in the moment. If the baby is blue, turn up the ventilator to pink up and stabilize the baby. Sounds good at the moment, but when the baby begins to crash again, the ventilator has to be cranked up more. This cycle is deadly and eventually the baby either finally crashes or permanent damage is done to the lungs eventually causing death.
This is one of Dr. Kays major differentiators in that he uses gentle ventilation techniques. Not only that, he is not overly aggressive in his approach. He looks to the future condition of the baby, not just the current state. For example, just because the baby is slightly blue doesn’t mean that the most critical organ, the brain, isn’t receiving enough oxygen. Due to how the arteries branch off the heart, the brain receives first priority for blood, then the rest of the body. This means that you can stress the rest of the organs for a time to get you past those tough humps, without damaging the brain.
Another difference between him and other doctors is his approach to having one person driving the decisions instead of the baby being passed to different doctors for each specialty. Having that single point enables him to make the most educated decision at a moments notice, critical in CDH babies.
I also came to appreciate the fact that Dr. Kays has no ego. It’s not about him diving in there and “fixing” these kids. His approach is to give the baby the best environment he can for survivability and viability.
The success of the above practices and philosophies is affirmed with his patients having a 90% survival rate. And get this, that 90% is skewed considering he typically handles the most severe cases! Think about it. If you have a mild case of CDH and your local doctors say that they can take care of it with almost a 100% mortality rate, why go anywhere else? This is why Dr. Kays sees the most severe conditions of CDH. It’s the people that are given no hope by their local doctors and then search for an answer online and find it in Dr. Kays, who’s incredibly passionate about taking care of these kids.
Dr. Kays spent 3+ hours describing a multitude of scenarios and how he may look to resolve them. He then gave us some quantitative hope. Based on his best guess, he said that our baby girl has a 70-75% chance of survival. He also indicated a 70-75% chance, with no brain damage. Doctors in Colorado gave our baby girl, at best, a 20% chance of survival with no certainty about her quality of life. Wow, that’s a big difference.
At this point, I have no doubts about our commitment to having Dr. Kays take care of our little girl. No red flags here. Just total confirmation that we are making the right decision.
Dr. Kays then went on describing the babies that he’s currently taking care of. Three boys, one with .8 LHR, and two with .6 LHR, .2 less then our baby girl! He wanted us to go up to the NICU to see them. As heavy as this was going to be, we couldn’t say no. I just needed some time to catch my breath before we saw these precious babies.
We headed up to the NICU. He had us wait just inside while he confirmed with the families that it would be ok for us to come over and see them. I’m glad he did because I needed a moment to prepare for this.
Tina and I just stood there taking it in. There were a couple preemie babies that we could see. Wow, so tiny. It’s amazing how small these lives are. Man, it’s hard not to get emotional.
Dr. Kays returns and leads us over to the CDH beds. There we see the first boy hooked up to the ventilator. He was stable and doing well.
The next baby we saw was surrounded by his family. Dr. Kays introduced us to the couple and their two other young children! I can only imagine how hard it would be to go through something like this with two other children to take care of as well. Tina was so overwhelmed with emotion that she couldn’t talk. I was able to squeak out a “Hi” but that was about it.
We then went to see the last baby boy. He just had his breathing tubes removed the day before and he was breathing on his own. This was one of the .6 LHR babies too! Dr. Kays motioned for us to come over closer. What happened next was amazing. That baby totally responded to Dr. Kays voice. No doubt that he spent a lot of time taking care of this baby.
We then met a few of the nurses who would probably be there when we have our baby girl. The whole team was incredibly warm and receptive. Dr. Kays then lead us down to the main lobby area.
On the way, I confirmed to him that is was no accident that we were here. He asked, “What do you mean?” I said that I have no doubt that we are supposed to be here. It’s not about luck, or “bad luck” as the other doctors we saw had put it. I know with every fiber in my being that God is sovereign and in control and that He has a purpose for this. I think my passion took him by surprise a bit, but he affirmed what I said.
I do know that God has a purpose and a plan for this. It’s not for me to know how it’s going to turn out, it’s my job to put all my trust in Him during this tough time.

